Latest News
- Clues beginning to emerge on asymtomatic SARS-CoV-2 infection
- Back in November of 2020, during the first wave of the COVID-19 pandemic, I was teaching an in-person microbiology laboratory. One of my students had just been home to see his parents, and they all c…
- Read more
- Could there maybe be better uses of genetics and probiotics?
- Professor Meng Dong and his laboratory have created a probiotic that can metabolize alcohol quickly and maybe prevent some of the adverse effects of alcohol consumption. The scientists cloned a highl…
- Read more
- ChatGPT is not the end of essays in education
- The takeover of AI is upon us! AI can now take all our jobs, is the click-bait premise you hear from the news. While I cannot predict the future, I am dubious that AI will play such a dubious role in…
- Read more
- Fighting infections with infections
- Multi-drug-resistant bacterial infections are becoming more of an issue, with 1.2 million people dying of previously treatable bacterial infections. Scientists are frantically searching for new metho…
- Read more
- A tale of two colleges
- COVID-19 at the University of Wisconsin this fall has been pretty much a non-issue. While we are wearing masks, full in-person teaching is happening on campus. Bars, restaurants, and all other busine…
- Read more
( 13863 Reads)
|So, now you know that being awash in information is a double-edged sword. I have shown you the types of information at your fingertips, what’s most reliable and why, and I have given you a blueprint for how to manage it all and find the truth. We end this chapter by looking at a few examples that show you how to use these methods.
Vaccines and autism
We began this chapter by showing the harm that has been caused by a small proportion of the population losing their trust in the MMR vaccine. Where did this mistrust originate? Autism Spectrum Disorder (ASD) is a horrible disease, and its symptoms typically appear between one to three years, which is also the time when many children are getting their initial vaccines. A diagnosis of ASD at the time of vaccination makes many parents jump to the conclusion that vaccination had some role in the precipitation of autism. This concern was certainly worthy of investigation. No health authorities would want to ignore the possibility that vaccines cause harm.
In 1998, Dr. Andrew Wakefield published on his work examining children who had ASD symptoms and whose parents blamed the MMR vaccine for the problem. The paper dropped a bombshell. It suggested a link between the MMR vaccine, a new inflammatory bowel disease discovered by the research, and the onset of ASD. The research article added fuel to a movement against vaccination that was beginning to gain a following. Vaccination rates in Briton dropped from 92% to below 80%, resulting in the return of measles epidemics in England and Wales. Fear of vaccination has now spread worldwide, and Public Health Departments are in a battle with the anti-vaccine movement to get vaccination rates back up to protective levels.
None of this had to happen. The Wakefield paper is remarkably flawed and should have never been accepted for publication. Let’s apply our recipe of truth and see if we can find the flaws.
First, what’s the sample size? The study group was small (n=12). A small group makes statistical analysis difficult, especially when drawing correlations between MMR, ASD, and a new bowel disease. This small sample size should have immediately raised concerns. In addition, after publication, investigators found that the authors cherry-picked the data included in the study to support their pet conclusions.
Second, this was just a correlation. While there was evidence for a new bowel disease, it was unclear how this could cause ASD. Even worse, the study claimed that ASD symptoms occurred immediately after the MMR injection. The original study trusted the parent’s recollection that symptoms of ASD appeared after the MMR vaccine. Later examination of the medical records indicated this wasn’t the case, with some ASD symptoms being mentioned by parents before vaccination and some occurring months later.
Third, look for flim-flam. GI inspections done by hospital pathologists reported the GI to be normal, but the study team later changed these to abnormal. These changes are very serious because they are an outright falsification of data.
Fourth, follow the money. The most damning revelation was that Wakefield had failed to disclose a financial conflict of interest. He had been funded by lawyers who were preparing a case against the manufacturer of the vaccine.
This minor paper in The Lancet medical journal will go down in history as one of the worst examples of scientific fraud. Scientists spent years, and a great deal of time and money, investigating vaccines and autism. The overwhelming consensus of numerous studies is that there is no link or any causal relationship. Governments wasted scarce funding for medical research on a wild goose chase. Thousands of parents were frightened into not vaccinating their children, and many of them suffered from preventable diseases. We are still fighting the effects of this paper, and the misinformation it spread decades later. Some of the blame falls on the public. We, as a society, have to work harder; finding the truth matters. Recently, the anti-vaccine movement had a terrible and unfortunate impact on the COVID-19 pandemic, causing too many people to refuse to get vaccinated. Zhong et. al estimate that the lack of vaccine coverage in the United States led to over 300,000 preventable deaths from COVID-19. One caveat is that the Zhong article still needs to undergo peer review.
Probiotics
Thirty years ago, scientists thought the bacteria that lived on humans were mostly harmless and somewhat beneficial to the host. However, this benefit was principally from helping to train the immune system and taking up space that pathogens might otherwise occupy. An important function, but thought not to be that consequential. A few researchers started to do experiments with specific strains of bacteria. These strains were demonstrating a positive effect, but scientists not involved in the research were skeptical, and the field seemed to belong with acupuncture, aromatherapy, and divination. While my view wasn’t that harsh, I will admit to not recognizing the importance of this topic to human health.
In 2007, a landmark experiment by Sinead Corr and coworkers demonstrated that a Lactobacillus salivarius strain could protect mice against infection with Listeria monocytogenes. Listeria infection can cause a disease that, once established, can have a mortality rate as high as 50%. In this elegant series of experiments, the authors first show that feeding mice L. salivarius for three days protected the mice from L. monocytogenes infection, decreasing the numbers of bacteria infecting the spleen and liver by over 10-fold. They then hypothesized that a small antimicrobial peptide that L. salivarius made, a bacteriocin, was the cause of the protection. In addition, a mutant L. salivarius strain that was unable to make the bacteriocin no longer conferred protection against L. monocytogenes.
Let’s again apply our recipe of truth to this experiment.
What’s the sample size? The experiments use five mice per strain tested. So for many of the tests, that is 10 to 40 mice - a small number. However, given the size of the effect, a 10 to 100 fold decrease in L. monocytogenes infection, that is sufficient to give the results statistical power. They used the T-test, which requires a normal distribution, and they certainly had a normal distribution if you look at the error bars. The resulting p-values were in the 0.001 to 0.05 range, meaning that at least 95% of the time, the difference between their tests and the controls is significant. So, the sample was big enough to show an effect. However, this is merely correlational. If L. salivarius is present, it inhibits L. monocytogenes. What makes this paper so good is they take it to the next level.
What’s the cause? It turns out L. salivarius is known to secrete bacitracin, an antimicrobial peptide, and the researchers hypothesized that it was the cause of the inhibition. To test this idea, they mutated L. salivarius and created a strain that could no longer make bacitracin and then used it in the same experiment they used with normal L. salivarius. It showed that the strain was no longer protective against L. monocytogenes. They also purified bacitracin from L. salivarius and showed the purified peptide could inhibit L. monocytogenes.
Follow the money. Who supported the research? At the end of the paper, they state that the government of Ireland provided funding for the work. I can see no reason that demonstrating this probiotic effect would be of any financial or other benefits to the researchers or the government of Ireland. There was no conflict of interest. In this paper, Corr and coworkers definitively demonstrate that microbes can have a probiotic effect and discover the cause of the probiotic effect through some elegant experiments.
A large body of further research supports the existence of probiotics. Other microbes can prevent or modulate certain infections. Probiotic bacteria also stimulate the immune system, aid digestion, and modulate the pH of the gut. The microbiome inhibits inappropriate inflammation (when the immune system attacks harmless factors in the body). The human microbiome’s effect on inflammation can even have a protective effect on bones.
As one example of an important bacterium, a newly discovered anaerobe, Akkermansia muciniphila, is a critical part of our gut microbiome. It is part of a handful of bacteria found in all humans and constitutes 0.5 to 5% of the bacteria found in the intestines. The presence of A. muciniphila has numerous protective effects. People in several unhealthy states (obesity, type 2 diabetes, inflammatory bowel disease, hypertension, and liver disease) contain lower concentrations of A. muciniphila. Also, several interventions that are known to help treat diabetes, such as metformin administration and bariatric surgery, also increase the population of A. muciniphila. There is a large body of evidence that suggests that the presence of this bacterium can protect against metabolic disorders and heart attacks. Your body even recruits this microbe to your gut by producing mucin, its preferred food. Thus, the bacterium does not rely on your diet for its nutrients.
Many of the positive effects of A. muciniphila stem from its ability to prevent weight gain. Feeding mice a diet that mimics a human western diet, high in fat and low in fiber, will cause them to gain excess weight much as humans do. However, if one group also consumes A. muciniphila, they have a 50% lower body weight gain when compared to a control group. The presence of A. muciniphila restores mucus production, causes the production of antimicrobial peptides, and increases the production of anti-inflammatory lipids. Also, killing the microbe by autoclaving eliminates its protective effects, which indicates that the bacterium has to be active and growing to have its positive impact. How A. muciniphila causes these responses in the intestine is still unknown, but the development of a probiotic may be coming soon.
A large body of work has shown that there are numerous probiotic bacteria. Proper administration of probiotics could bring potential health benefits. Food manufacturers have taken notice and jumped on the probiotic bandwagon hawking products of dubious quality. Lactobacillus and Bifidobacterium are the most popular genera today for formulating probiotic foods, but it is unclear if these formulations are beneficial. If you are interested in probiotics, and I do think there are reasons to be, be wary and choose those products that have actual scientific experiments behind them.
Exercise will not help you lose weight
In the United States, two-thirds of the adult population is overweight, with one-third being obese, making it a vital public health concern. It is not just the US; over 600 million adults, and 100 million children, are obese worldwide. Obesity increases risk factors for cardiovascular disease, type 2 diabetes, high blood pressure, and joint problems. Medical costs associated with obesity are estimated to be $140 billion annually. The military even sees the obesity epidemic as a security risk, turning away many recruits because they weigh too much. America needs to lose weight!
To combat this problem, health experts have recommended higher physical activity and a healthy diet containing more fruits and vegetables and less processed food, but is it that simple? Ironically, headlines in the last few years in Vox, The Washington Post, The Telegraph, and The LA Times scream that exercise does not help you lose weight. Several studies in the last decade have found a weak link between physical activity and weight loss. From this, many have concluded that exercise will not help you lose weight. What discouraging news, but is it true? It seems counter-intuitive that burning more calories does not help. What’s going on?
If you spend some time digging into the studies, especially looking at the methods used, you find some critical caveats. First, the research involves humans, and as such, controlling confounding variables is much more challenging than in animal models. Imagine you want to study the effect of adding a walking regime to a program where overweight individuals are trying to lose weight. You want to know each person’s food intake and then split them into groups where one group walks and the other does not. In most cases, surveys measure food intake. Using a survey has two issues. One, you depend upon the participants to be capable of measuring correctly the food they eat. Since food labels can have caloric measurement errors of up to 20%, this can be more difficult than many people anticipate. Two, you are trusting participants to be honest and chart everything. They may forget to log that cookie they had at a work meeting. That could have been an extra 100 calories and can make a huge difference. You are also counting on people to exercise, and the best studies will directly supervise the exercise sessions to verify participation. A perfect study would house the participants for the duration of the investigation and monitor every morsel they consumed. This type of experiment would be difficult due to its cost.
Another problem with many of these studies is that the definition of physical activity can mean anything from gardening to walking, to high-intensity interval training. Studies have used walking (> 8,000 steps a day), aerobic exercise (heart rate at 60% of maximum), high-intensity aerobic exercise (70% or greater of max heart rate), and resistance training (challenging your muscles to move things). Not surprisingly, how your body responds to exercise is dependent upon the exercise that you do. When many folks exercise, they will burn 200-500 calories and are hungry when they get done. If you immediately eat the wrong thing, a jelly donut, you have wiped out any gain the exercise gave you. Caloric compensation is especially a problem with moderate exercise. If you walk or jog lightly, your body will empty the contents of your stomach in preparation for more food. In contrast, if you exercise at a 70% effort, there is a delay in stomach emptying, and thus a delay in hunger. Most studies use moderate exercise and hence make it more difficult to resist eating.
If you chart each person in a weight-loss study, instead of focusing on the overall average, there is a wide variation in their success (Figure 2.10). In one study, the average weight loss was 3.8 kg (8.3 pounds) in 12 weeks. That is excellent progress. However, if you chart the results, you can see there is a wide range of success from losing 14.3 kg to gaining 3 kg. Even in closely monitored studies using intense exercise (>70% effort), some folks lose weight while others may gain weight! Why? Investigation of these non-performers found a series of compensatory behaviors. They would eat more calories to make up for the ones spent on exercise, or they would decrease their regular activity outside of the exercise sessions, causing their overall calorie expenditure during the day to not increase much.
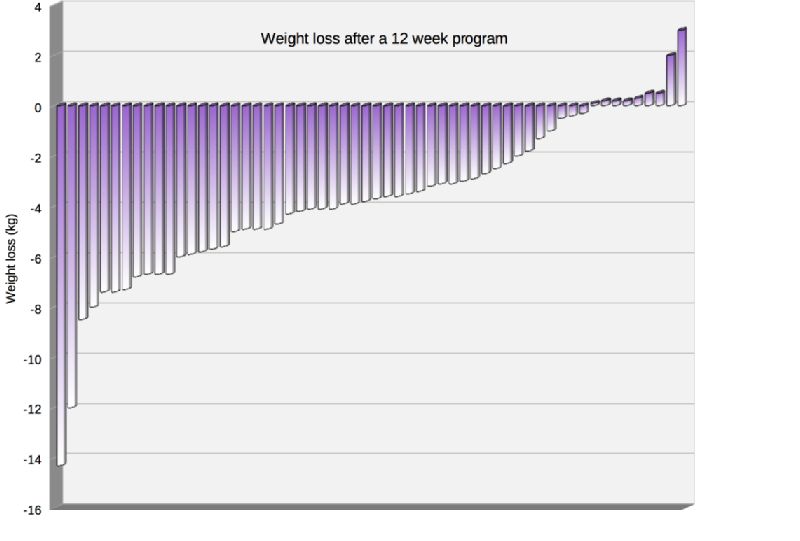
Figure 2.10. Weight loss of individuals in a twelve-week weight reduction program.. The success in most weight loss programs is highly dependent upon the individual. In this study, researchers monitored the amount of exercise closely, but nothing else. Data adapted from Figure 1 of King NA, Hopkins M, Caudwell P, Stubbs RJ, Blundell JE. 2009. Beneficial effects of exercise: Shifting the focus from body weight to other markers of health. Br J Sports Med 43:924–927.
The take-home message here is that there is a variable success in losing weight with exercise. The popular press unfortunately latched on to the people who failed. The scientists and the scientific studies showed a range of weight loss, but this subtlety got lost in the translation of the research to the general public. To be fair to the press, many of the best articles did point out that exercise alone will not get you to your weight loss goals. Research shows that long-term, consistent efforts where a person both exercises, eats well, and works on the psychological aspects of eating are successful. A person who wants to lose weight and keep it off learns to resist the temptation of food and shows discipline and restraint in their eating habits. Indeed, you cannot outrun a bad diet. It is still an open question as to what exercise and what intensity is best for weight loss, but exercise does play an important role. No matter what the current findings indicate about weight loss, higher rates of physical activity have numerous physical and mental health benefits and should continue.
This example demonstrates that it is essential to see past the headlines and dig into the details. If you only read one press article on the topic, you may walk away, seeing little benefit to exercise. However, if you read more widely, you would find numerous well-written articles; the one in Vox is exceptionally good and gives a more balanced view. If you then investigate weight loss in the primary literature, you would develop a much more nuanced view and even learn behaviors that could make your weight loss journey a success. (Although, I am not saying you need to lose weight. You look great!)
I hope this chapter has shown you a toolset you can apply to any subject you are learning. Be curious, be skeptical, be open to change, read widely, and read critically.
Most importantly, think well and think for yourself. Don’t let anyone make up your mind for you. The world needs independent thinkers.